
Authors: Janice Eng, Dominik Zbogar | Published: 7 July 2025
Lending a hand to build SCI expertise in the Ukraine
We spoke to Dr. Andrei Krassioukov, Physiatrist in the Spinal Cord Program at Vancouver Coastal Health’s GF Strong Rehabilitation Centre.

Dr. Andrei Krassioukov, a rehabilitation physician with GF Strong Rehab Centre, clinician-researcher at the International Collaboration on Repair Discoveries (ICORD), as well as an expert contributor for the SCIRE Project, has been volunteering his time in Ukraine over the last two years.
Assembled by the World Health Organization, health care professionals in medicine, physical therapy, occupational therapy, nursing, and psychology have visited war zones on multiple occasions to establish a specialized national spinal cord injury centre in the Rivne region of Ukraine. Amidst the ongoing war, the number of patients with spinal cord injuries and other catastrophic injuries continues to increase. Spinal cord injury is a particularly specialized area of medicine so supplies, person power, and medical expertise are sorely needed.
Can you describe your role as a healthcare provider and World Health Organization representative in the Ukraine?
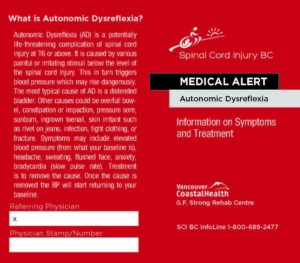
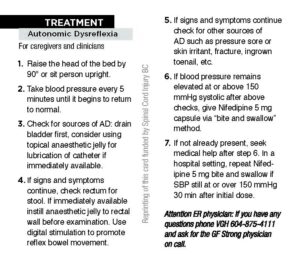
“It was mostly training, training, training clinicians. I had daily meetings with medical staff. We attended every morning clinical round on the acute wards and spinal cord wards.” Dr. K (how most people refer to him) taught clinicians how to conduct spinal cord injury assessments, using the International Standards for Neurological Classification (ISNCSCI). He provided training on autonomic dysreflexia, as well as bowel and bladder management. He led sessions on the management of spasticity after spinal cord injury, including how to use botulinum toxin injections and monitoring outcomes with muscle electromyography.

Ukraine street mural, as photographed by Dr. K. on April 12, 2024
What are some of the greatest challenges you have seen?
“Resources were scarce with only a few vials of botulinum toxin available per month. They were fortunate to get some international donations of botulinum toxin which helped to stretch their supplies. Most of these young people had multiple traumas, and their injuries are more complex than what we would see in a typical car accident. As the war has caused so much destruction, some people we discharge no longer have a place to go home to. Many people in Ukraine are already affected by depression, anxiety, and post-traumatic stress from the long war effort. This centre has brought in new resources for psychological support for coping with the devastating effects of these injuries and personal circumstances.”
What stood out for you the most during your time in the Ukraine?
“The work was stressful with continual alerts, bombings nearby, and evacuations to shelters, but not compared to the stress that Ukrainians have had to endure. What stood out for me was the humanity and resilience of the Ukrainian people who managed to find some happiness in moments of their life during the ongoing war. I saw this resiliency in the soldiers recovering from their injuries, and from the everyday people that I have met.”
The Spinal Cord Centre now has 100 beds and will serve as a model for similar facilities in other regions of Ukraine. We thank Dr. Krassioukov and all health care professionals who have been courageous enough to lend a hand during traumatic times.
![]()

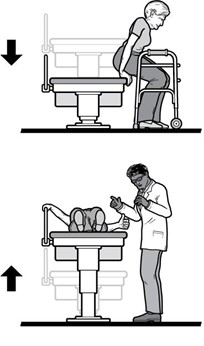
 Primary care providers (PCPs) take care of the day-to-day health of people at all stages of life. They are often the first contact when someone has a non-emergency health concern. This person is often a family doctor, but the role can also be filled by a nurse practitioner, physician assistant. They play a central role in the care team for people with spinal cord injury (SCI) and you will maintain a relationship with your PCP for many years. The responsibilities of a PCP include:
Primary care providers (PCPs) take care of the day-to-day health of people at all stages of life. They are often the first contact when someone has a non-emergency health concern. This person is often a family doctor, but the role can also be filled by a nurse practitioner, physician assistant. They play a central role in the care team for people with spinal cord injury (SCI) and you will maintain a relationship with your PCP for many years. The responsibilities of a PCP include: Go to the emergency room or call your regional emergency number if…
Go to the emergency room or call your regional emergency number if…


 If your PCP is interested in more in-depth information, case studies, advice, and guidelines for these checklists and SCI-specific care, they can check out the
If your PCP is interested in more in-depth information, case studies, advice, and guidelines for these checklists and SCI-specific care, they can check out the 

 Employment
Employment Social support refers to one’s relationships with other people, and the interactions, support, and care provided by this network of people, including family members, friends, and peer community. There is consistent evidence that more social support is linked to higher QoL in people with SCI.
Social support refers to one’s relationships with other people, and the interactions, support, and care provided by this network of people, including family members, friends, and peer community. There is consistent evidence that more social support is linked to higher QoL in people with SCI.
 I was skiing when I broke my neck. I had just turned 19, living in Vancouver. I went on a run that was steep and ended up going quite fast and then crashing. Somewhere in the whole thing I felt my neck break. I experienced it as feeling my body was expanding, the size of the universe. I experienced it as a sound like multiple sirens going off, very loud noises going very broadly. Then, I experienced my body going into a fetal position but when I opened my eyes my arms were up here. I said to myself, “You broke your neck – don’t move.” Eventually, people went down and got a piece of plywood to carry me off the mountain. They took me down, sort of bouncing, which is probably where more damage came.
I was skiing when I broke my neck. I had just turned 19, living in Vancouver. I went on a run that was steep and ended up going quite fast and then crashing. Somewhere in the whole thing I felt my neck break. I experienced it as feeling my body was expanding, the size of the universe. I experienced it as a sound like multiple sirens going off, very loud noises going very broadly. Then, I experienced my body going into a fetal position but when I opened my eyes my arms were up here. I said to myself, “You broke your neck – don’t move.” Eventually, people went down and got a piece of plywood to carry me off the mountain. They took me down, sort of bouncing, which is probably where more damage came.
 So then, we went into sailing through
So then, we went into sailing through 




 We were able to put on the Public Salons for about four or five years, having received a million dollars from a foundation in California. We tried to raise additional money to bolster that, but eventually we ran out. We had to try to make it profitable on its own, but it wasn’t designed for fundraising, it was designed for giving me pleasure. Fundraising would be a real challenge. So, we had to totally revolutionize it a couple years ago. What I do now is bring in an international speaker, that’s the star, and then have local responders who give them questions, comments, critiques, etc. So that’s the new model and it seems to be working. I brought in a former chief planner of the World Bank, Alain Bertaud, and a recent Think-Tank Salon included experts on addiction and mental health. In a way, I’m still on those two issues of prices and addiction, now attacking them from outside, not from the inside as mayor.
We were able to put on the Public Salons for about four or five years, having received a million dollars from a foundation in California. We tried to raise additional money to bolster that, but eventually we ran out. We had to try to make it profitable on its own, but it wasn’t designed for fundraising, it was designed for giving me pleasure. Fundraising would be a real challenge. So, we had to totally revolutionize it a couple years ago. What I do now is bring in an international speaker, that’s the star, and then have local responders who give them questions, comments, critiques, etc. So that’s the new model and it seems to be working. I brought in a former chief planner of the World Bank, Alain Bertaud, and a recent Think-Tank Salon included experts on addiction and mental health. In a way, I’m still on those two issues of prices and addiction, now attacking them from outside, not from the inside as mayor.
 Ainsley is 17 and plans on doing a Bachelor of Arts at the University of British Columbia after graduating high school this year!
Ainsley is 17 and plans on doing a Bachelor of Arts at the University of British Columbia after graduating high school this year! Dan is 37 and a full-time student at Douglas College in Recreation Therapy! He enjoys cooking and has a dog.
Dan is 37 and a full-time student at Douglas College in Recreation Therapy! He enjoys cooking and has a dog. Caleb is 35 and likes to spend his time outdoors and doing sports like scuba diving, whitewater kayaking and sitskiing!
Caleb is 35 and likes to spend his time outdoors and doing sports like scuba diving, whitewater kayaking and sitskiing!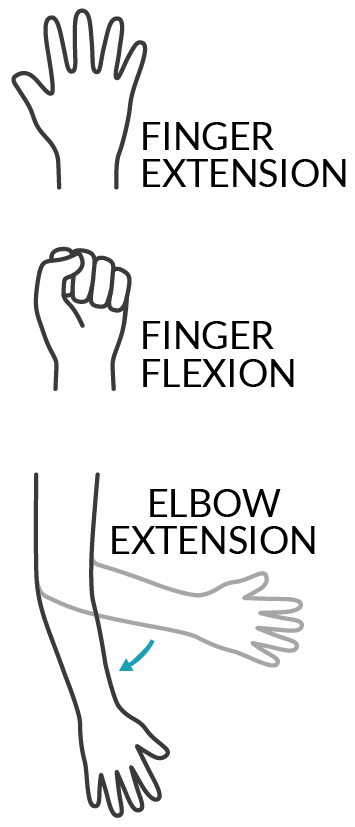
 This was very true for Dan. After his nerve transfer surgery, he lost some muscle strength in his left hand and arm. He was still strong enough to push his chair but not to stop. As a result, he went from strictly using a manual chair to using a power wheelchair for about 10 months. The rest of Dan’s recovery did not go so smoothly either. He explains, “in my left arm, when I moved my arm in a certain way, I would get a twang. It felt like I hit my funny bone but times 100. It was really bad and that lasted about two weeks. I also had some numbness in my left thumb all the way down to my palm. I still have numbness but it’s mostly the tip of my thumb so it’s better.” On top of everything, Dan was living at home and not at a rehabilitation centre when he had his surgeries. He came to realize post-surgery that he did not have all the necessary supports in place to accommodate the temporary losses in function. Reflecting on these struggles, he suspects that since people with chronic SCI don’t get nerve transfers often, there is less awareness of how much the surgery can affect their functional abilities.
This was very true for Dan. After his nerve transfer surgery, he lost some muscle strength in his left hand and arm. He was still strong enough to push his chair but not to stop. As a result, he went from strictly using a manual chair to using a power wheelchair for about 10 months. The rest of Dan’s recovery did not go so smoothly either. He explains, “in my left arm, when I moved my arm in a certain way, I would get a twang. It felt like I hit my funny bone but times 100. It was really bad and that lasted about two weeks. I also had some numbness in my left thumb all the way down to my palm. I still have numbness but it’s mostly the tip of my thumb so it’s better.” On top of everything, Dan was living at home and not at a rehabilitation centre when he had his surgeries. He came to realize post-surgery that he did not have all the necessary supports in place to accommodate the temporary losses in function. Reflecting on these struggles, he suspects that since people with chronic SCI don’t get nerve transfers often, there is less awareness of how much the surgery can affect their functional abilities. Ainsley is now 2 years after the nerve transfers and has gained the ability to fully open both hands. On the left, her restored hand closing from nerve transfer is very strong and she can pick things up. The right-hand pinch gained from the tendon transfer is functional and continues to build strength. All these improvements in her fingers and hands mean that Ainsley can use her cell phone with finger gestures, scratch an itch, adjust her hair, and hold and use things like cutlery, a toothbrush, makeup, and bank cards. The triceps nerve transfer has recovered to the point where she can now extend both arms against gravity. These days, Ainsley is getting ready to hit the road in a custom hand control vehicle, something that would not have been possible if not for the triceps surgeries that improved her strength enough to turn a steering wheel. Hopeful for the future, Ainsley says that she is “still improving everyday”.
Ainsley is now 2 years after the nerve transfers and has gained the ability to fully open both hands. On the left, her restored hand closing from nerve transfer is very strong and she can pick things up. The right-hand pinch gained from the tendon transfer is functional and continues to build strength. All these improvements in her fingers and hands mean that Ainsley can use her cell phone with finger gestures, scratch an itch, adjust her hair, and hold and use things like cutlery, a toothbrush, makeup, and bank cards. The triceps nerve transfer has recovered to the point where she can now extend both arms against gravity. These days, Ainsley is getting ready to hit the road in a custom hand control vehicle, something that would not have been possible if not for the triceps surgeries that improved her strength enough to turn a steering wheel. Hopeful for the future, Ainsley says that she is “still improving everyday”. Dan is coming up on 3 years after the nerve transfers. Although his grip is not strong, it is strong enough that he can use and squeeze the brakes on the new e-bike attachment for his wheelchair, which he would not have been able to do without the nerve transfer. Being able to extend his fingers has made it much easier to open his hand to grasp things and move them around. He has more function in his hands then before, but he still has not recovered some of the strength he lost after the surgeries. Dan described how “Before the surgery I could lift a full backpack of groceries off of the back of my chair now I have difficulty if there’s any weight in my bag.” That said, he is still waiting to see how much he improves, explaining, “…it’s coming, it’s just not there yet. I think they say the plateau is four years for this surgery…”, referencing experts who say that improvements for nerve transfers typically reach their peak at around 4 years.
Dan is coming up on 3 years after the nerve transfers. Although his grip is not strong, it is strong enough that he can use and squeeze the brakes on the new e-bike attachment for his wheelchair, which he would not have been able to do without the nerve transfer. Being able to extend his fingers has made it much easier to open his hand to grasp things and move them around. He has more function in his hands then before, but he still has not recovered some of the strength he lost after the surgeries. Dan described how “Before the surgery I could lift a full backpack of groceries off of the back of my chair now I have difficulty if there’s any weight in my bag.” That said, he is still waiting to see how much he improves, explaining, “…it’s coming, it’s just not there yet. I think they say the plateau is four years for this surgery…”, referencing experts who say that improvements for nerve transfers typically reach their peak at around 4 years. Even though Caleb is only 1 year and 3 months after the nerve transfer and still has a long way to go, he is already happy with the improvements. “Going from zero movement in my fingers to now, it’s kind of huge”. The first big impact the nerve transfers had in Caleb’s day-to-day life was probably around four months in, when he was able to open his hand to grab his toothbrush without any kind of assistance. He can now grab a toothbrush or pop can and hold on to it without a problem. His triceps progress has been harder to pin down. There is some movement in his left arm and a small amount in his right arm but he wonders if that would have come back naturally after SCI regardless of the nerve transfers. Whether or not the improvements came from the nerve transfers or from natural recovery, it has been a big help for Caleb’s mobility and being able to shift and transfer.
Even though Caleb is only 1 year and 3 months after the nerve transfer and still has a long way to go, he is already happy with the improvements. “Going from zero movement in my fingers to now, it’s kind of huge”. The first big impact the nerve transfers had in Caleb’s day-to-day life was probably around four months in, when he was able to open his hand to grab his toothbrush without any kind of assistance. He can now grab a toothbrush or pop can and hold on to it without a problem. His triceps progress has been harder to pin down. There is some movement in his left arm and a small amount in his right arm but he wonders if that would have come back naturally after SCI regardless of the nerve transfers. Whether or not the improvements came from the nerve transfers or from natural recovery, it has been a big help for Caleb’s mobility and being able to shift and transfer.
 Staying physically active after SCI is important for your health. There is moderate to strong evidence that physical activity has many benefits after SCI including:
Staying physically active after SCI is important for your health. There is moderate to strong evidence that physical activity has many benefits after SCI including: Athlete Classification
Athlete Classification
 Upright cycles
Upright cycles Tandem bikes
Tandem bikes Arm cycle add-ons
Arm cycle add-ons If you are looking to go on some trails, an off-road wheelchair may appeal to you. These wheelchairs are used for recreational riding, such as going for a hike, or going fishing. Off-road wheelchairs often have larger, knobbier tires that are meant to withstand the trail, roots, and rocks. Like the arm-cycles, off-road wheelchairs come in a variety of set ups. Some setups may look like a typical manual wheelchair, but with larger wheels. There are also ones that are controlled with push-levers (such as the
If you are looking to go on some trails, an off-road wheelchair may appeal to you. These wheelchairs are used for recreational riding, such as going for a hike, or going fishing. Off-road wheelchairs often have larger, knobbier tires that are meant to withstand the trail, roots, and rocks. Like the arm-cycles, off-road wheelchairs come in a variety of set ups. Some setups may look like a typical manual wheelchair, but with larger wheels. There are also ones that are controlled with push-levers (such as the 
 For those who are interested in competition, wheelchair racing may be an option. Wheelchair race events range from the 100m, 200m, 400m, 800m, 1500m, and 5k distance races in track and field, to marathons. Racing wheelchairs differ from the wheelchairs and cycles listed above in that they typically have two wheels with a third one extended out in front. Ideally, race chairs should be light-weight to enhance performance. When seated, the wheelchair should fit “like a glove”, and there should be little movement in the seat. Unlike arm-cycles, the feet are bent down and kept closer to the body. In addition, specialized rubber gloves are worn to push the rims during races.
For those who are interested in competition, wheelchair racing may be an option. Wheelchair race events range from the 100m, 200m, 400m, 800m, 1500m, and 5k distance races in track and field, to marathons. Racing wheelchairs differ from the wheelchairs and cycles listed above in that they typically have two wheels with a third one extended out in front. Ideally, race chairs should be light-weight to enhance performance. When seated, the wheelchair should fit “like a glove”, and there should be little movement in the seat. Unlike arm-cycles, the feet are bent down and kept closer to the body. In addition, specialized rubber gloves are worn to push the rims during races. Wheelchair tennis is played on the same court as able-bodied tennis, and with similar rules. One rule difference is that in wheelchair tennis, players are allowed two bounces instead of one, and the second bounce can be anywhere – even out of bounds. Although one can play wheelchair tennis in their day chair, tennis wheelchairs are often preferred during play. These wheelchairs are faster, lighter, more agile, and more stable. The wheels on the wheelchair are also angled (i.e., there is more camber ) to allow for more swift turning. For those with limited hand function, taping the racquet to your hand is common practice, though it can take some time to find the optimal tension for you. Therefore, people with all levels of ability can play wheelchair tennis.
Wheelchair tennis is played on the same court as able-bodied tennis, and with similar rules. One rule difference is that in wheelchair tennis, players are allowed two bounces instead of one, and the second bounce can be anywhere – even out of bounds. Although one can play wheelchair tennis in their day chair, tennis wheelchairs are often preferred during play. These wheelchairs are faster, lighter, more agile, and more stable. The wheels on the wheelchair are also angled (i.e., there is more camber ) to allow for more swift turning. For those with limited hand function, taping the racquet to your hand is common practice, though it can take some time to find the optimal tension for you. Therefore, people with all levels of ability can play wheelchair tennis. Basketball
Basketball Wheelchair rugby was developed specifically for people with tetraplegia and has grown to include people without SCI but with similar functional abilities (e.g., some impaired arm and hand function in addition to impaired leg function). Wheelchair rugby is played with a volleyball. The goal of the game is to carry the ball over the other team’s goal line. Unlike able-bodied rugby, wheelchair rugby is played indoors on a court. Specialized wheelchairs are used to play wheelchair rugby and can be separated into chairs for offensive players and chairs for defensive players. Offensive wheelchairs are set up for speed and mobility and are distinguished with a front bumper to prevent other chairs from hooking them. Often, offensive chairs are used by players with more function. On the other hand, defensive wheelchairs are set up with a bumper to hook and hold onto other players. Defensive chairs are often used by players with less function. Additional equipment used in rugby include straps and gloves. Straps are used on the waist (to compensate for a lack of core muscles), the thighs (to prevent them from falling to the side or from shifting side to side), and the feet (for comfort). Meanwhile, gloves work to protect the skin, add extra grip when pushing the chair, and to making throwing and catching the ball easier.
Wheelchair rugby was developed specifically for people with tetraplegia and has grown to include people without SCI but with similar functional abilities (e.g., some impaired arm and hand function in addition to impaired leg function). Wheelchair rugby is played with a volleyball. The goal of the game is to carry the ball over the other team’s goal line. Unlike able-bodied rugby, wheelchair rugby is played indoors on a court. Specialized wheelchairs are used to play wheelchair rugby and can be separated into chairs for offensive players and chairs for defensive players. Offensive wheelchairs are set up for speed and mobility and are distinguished with a front bumper to prevent other chairs from hooking them. Often, offensive chairs are used by players with more function. On the other hand, defensive wheelchairs are set up with a bumper to hook and hold onto other players. Defensive chairs are often used by players with less function. Additional equipment used in rugby include straps and gloves. Straps are used on the waist (to compensate for a lack of core muscles), the thighs (to prevent them from falling to the side or from shifting side to side), and the feet (for comfort). Meanwhile, gloves work to protect the skin, add extra grip when pushing the chair, and to making throwing and catching the ball easier.

 Alpine skiing, also known as downhill skiing, is a sport that individuals with tetraplegia and paraplegia can partake in with the use of sit-skis. In general, sit skis have a bucket-type of seat with an adjustable seat and footrest. To create a smoother ride, sit-skis have additional features such as suspensions and a shock compression system under the seat. The seat and suspension/shock systems are all connected to either a single ski (mono-ski) or a pair of skis (bi-skis). In general, mono-skis require the user to have good upper body strength, and the ability to ski independently. Bi-skis are often used by individuals who may require some assistance. Often, bi-skis are used with an able-bodied individual who skis behind them. Skiers who use a sit-ski can use the typical chairlifts at the mountains and with experience, can access all terrains of ski areas.
Alpine skiing, also known as downhill skiing, is a sport that individuals with tetraplegia and paraplegia can partake in with the use of sit-skis. In general, sit skis have a bucket-type of seat with an adjustable seat and footrest. To create a smoother ride, sit-skis have additional features such as suspensions and a shock compression system under the seat. The seat and suspension/shock systems are all connected to either a single ski (mono-ski) or a pair of skis (bi-skis). In general, mono-skis require the user to have good upper body strength, and the ability to ski independently. Bi-skis are often used by individuals who may require some assistance. Often, bi-skis are used with an able-bodied individual who skis behind them. Skiers who use a sit-ski can use the typical chairlifts at the mountains and with experience, can access all terrains of ski areas. Cross Country Skiing
Cross Country Skiing Sledge (Ice) Hockey
Sledge (Ice) Hockey Community Voices: Terry
Community Voices: Terry
 Kayaks are available for people with all levels of SCI. While individuals with a lower level of injury may use non-adapted kayaks, adaptations are available for comfort and to accommodate those with limited function. Some kayaks may have custom seating with side and abdominal support. These supports are cushioned to protect the skin while kayaking. Stabilizing outriggers are available to increase stability of the boat and to reduce the chances of tipping. For those with limited arm/hand function, there are various adaptations for the paddle including:
Kayaks are available for people with all levels of SCI. While individuals with a lower level of injury may use non-adapted kayaks, adaptations are available for comfort and to accommodate those with limited function. Some kayaks may have custom seating with side and abdominal support. These supports are cushioned to protect the skin while kayaking. Stabilizing outriggers are available to increase stability of the boat and to reduce the chances of tipping. For those with limited arm/hand function, there are various adaptations for the paddle including:








 Duncan’s Experience
Duncan’s Experience






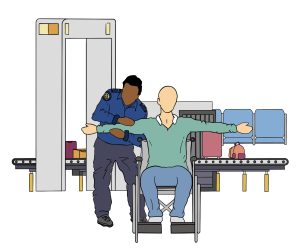
 When boarding the plane, you will usually be the first to board. This allows you extra time to transfer to your seat and to get comfortable without the pressure of other passengers waiting in the aisle behind you. Ask the airline about the boarding procedure, as it varies per airline. In general, you will remain in your wheelchair and travel to the door of the plane in it. You will then be transferred into an aisle chair. To facilitate the transfer, ensure you know how to guide the transfer through providing clear, verbal instructions to the airline staff. If you are unable to transfer from an aisle chair into your seat, some airlines have specialized slings that can be used to transfer you into your seat. Similar to the aisle chair, you will need to express your needs and guide your transfer from your wheelchair into the sling.
When boarding the plane, you will usually be the first to board. This allows you extra time to transfer to your seat and to get comfortable without the pressure of other passengers waiting in the aisle behind you. Ask the airline about the boarding procedure, as it varies per airline. In general, you will remain in your wheelchair and travel to the door of the plane in it. You will then be transferred into an aisle chair. To facilitate the transfer, ensure you know how to guide the transfer through providing clear, verbal instructions to the airline staff. If you are unable to transfer from an aisle chair into your seat, some airlines have specialized slings that can be used to transfer you into your seat. Similar to the aisle chair, you will need to express your needs and guide your transfer from your wheelchair into the sling. 
 As the plane begins to descend, remind the flight attendant that your wheelchair is underneath the plane, and needs to be brought to the door upon landing. During the decent, individuals with limited core function may have some difficulty bracing themselves in the seat. One participant from an interview study explained that it felt like their “body wanted to fling forward”. If you find yourself in this situation, some ways to stabilize yourself in the seat include bracing yourself against the seat in front of you, or hanging onto the arm rests. Some individuals also opt to use a chest strap/abdominal binder to help support their position in the seat during landing.
As the plane begins to descend, remind the flight attendant that your wheelchair is underneath the plane, and needs to be brought to the door upon landing. During the decent, individuals with limited core function may have some difficulty bracing themselves in the seat. One participant from an interview study explained that it felt like their “body wanted to fling forward”. If you find yourself in this situation, some ways to stabilize yourself in the seat include bracing yourself against the seat in front of you, or hanging onto the arm rests. Some individuals also opt to use a chest strap/abdominal binder to help support their position in the seat during landing.

 Being able to drive is an important skill that is helpful for day-to-day activities. Research has shown that being able to drive is related to many benefits, such as:
Being able to drive is an important skill that is helpful for day-to-day activities. Research has shown that being able to drive is related to many benefits, such as:





 ©Kevauto, CC BY-SA 4.0 7. Eighth-generation Civic sedan ©OSX, CC 0 8. Ford F-150 crew cab – 05-28-2011 ©IFVEHICLE, CC 0")



. Vehicle transfer and wheelchair loading techniques in independent drivers with paraplegia. Frontiers in Bioengineering and Biotechnology, 3(139), 1-7.")

 Decide where you will place your wheelchair: in the front passenger seat, or the back seats. Those with weaker shoulder muscles should consider loading their wheelchair into the front seats.
Decide where you will place your wheelchair: in the front passenger seat, or the back seats. Those with weaker shoulder muscles should consider loading their wheelchair into the front seats.






 After a spinal cord injury (SCI), there is often an increased need for social support and accessibility in the environment. Due to these factors, careful planning and consideration are required for optimal housing. Housing is an important factor in transitioning back into the community, which is a strong predictor of quality of life. Some (weak) evidence has noted that housing can influence quality of life as it:
After a spinal cord injury (SCI), there is often an increased need for social support and accessibility in the environment. Due to these factors, careful planning and consideration are required for optimal housing. Housing is an important factor in transitioning back into the community, which is a strong predictor of quality of life. Some (weak) evidence has noted that housing can influence quality of life as it:










 I work in acute care, so I primarily look after people with new injuries – they tend to be traumatic injuries from car accidents, falls, and sports. We also admit patients with spinal cord injury (SCI) from cancer as well as infections. The length of stay for patients varies from about 3 weeks and, in rare cases, up to a year. It’s about taking care of people and doing much more than just applying your knowledge and skills. People with SCI are in a tough spot, and don’t know what to do next. You need to connect with the person, help them be empowered and regain control of their life.
I work in acute care, so I primarily look after people with new injuries – they tend to be traumatic injuries from car accidents, falls, and sports. We also admit patients with spinal cord injury (SCI) from cancer as well as infections. The length of stay for patients varies from about 3 weeks and, in rare cases, up to a year. It’s about taking care of people and doing much more than just applying your knowledge and skills. People with SCI are in a tough spot, and don’t know what to do next. You need to connect with the person, help them be empowered and regain control of their life.

{kind=link}
{kind=link}
.jpg){kind=link}
_Boeing_757-2B7(SF)_C-FMEP_904_(9741592213).jpg){kind=link}
,_front_12.12.20.jpg){kind=link}
_VTi-L_sedan_(2015-07-09)_01.jpg){kind=link}
{kind=link}
{kind=link}
#/media/File:Google_Home_with_Home_Hub_and_Home_Mini_on_table.jpg){kind=link}