Author: Sharon Jang | Reviewer: Courtney Pollock | Published: 18 October 2023 | Updated: ~
Key Points
- Staying active after SCI has many benefits, but structured workouts may not be for everyone. Sports may be a good alternative to stay physically active.
- Adapted sports (sometimes called “adaptive sports”) are sports that use modified equipment to allow individuals of all abilities to participate.
- Participating in adapted sports is a great way to build social connections with others and to become a part of a community.
- There are a variety of sports that can be played including cycling, court sports, winter sports, and water sports. This article introduces various adapted sports and the required equipment to partake in them.
 Staying physically active after SCI is important for your health. There is moderate to strong evidence that physical activity has many benefits after SCI including:
Staying physically active after SCI is important for your health. There is moderate to strong evidence that physical activity has many benefits after SCI including:
- Allowing you to perform everyday activities (e.g., shopping, cooking, transferring) with more ease,
- Improving depression and quality of life,
- Increasing muscle strength and endurance,
- Management of blood sugar levels,
- Helping you to breathe with more ease,
- Reducing pain and spasticity.
Although going to a gym is one common way to get moving, there are a variety of adapted sports that can also be played. While this article discusses a selection of adapted sports (including handcycling, court sports, winter sports, and water sports), it should be noted that almost any sport can be adapted for participation after SCI.
Refer to our article on Physical Activity for more information!
Adapted sports are sports that can be played with equipment and approaches that are adapted to a person’s physical abilities. Many adapted sports have been altered in one of many ways to promote accessibility. Some of these adaptations include changes to the rules of a game, modifications in the equipment, or specialized equipment to allow you to partake in a sport.
 Athlete Classification
Athlete Classification
 Athlete Classification
Athlete ClassificationThere are different levels of adapted sports, ranging from recreational (or just for fun and fitness) to competition. Should you want to become competitive, classifications are used to ensure that competition is equal and fair. Classifications are used to determine which athletes should be grouped together. In adapted sports, classification is based on function (e.g., strength, how many limbs are affected by injury, range of movement, tone/spasticity). This is similar to categorizing by age, gender, or weight in able-bodied sports.
Precautions when trying new sports
While trying out new sports can be fun and exciting, skin health is an important consideration. Trialing new sports is often associated with trying new equipment. When trying new equipment, it is important to check for red marks or pressure spots on your skin including your seat and any area of the body positioned against equipment (e.g., footrest or frame). People will commonly use the cushion from their everyday chair in their sport chair when they first try a sport. However, it is important to remember that although it is the same cushion, you may be sitting in a different position (e.g., seat angle) which will change pressure and potential forces from rubbing. The best approach is like that of trialing a new wheelchair or cushion: frequently check your skin in the early days of your new sport. This means that it is best to start with shorter sessions and work your way up in time once you know that your skin can tolerate the new equipment and positions. In water sports such as kayaking, or in rainy conditions for outdoor sports, make sure to check your skin when you are done since being wet can make the skin more prone to injury.
Additionally, you may want to consider the influence of temperature (extreme hot or cold weather), as temperature regulation may be impaired with an SCI.
Refer to our article on Pressure Injuries for more information!
Handcycles are a type of bicycle that is propelled by the arms instead of the legs. There are different types of handcycles available for all levels of ability. In general, most arm-cycles have alternative handle options for those with limited hand function.

Types of arm cycles
Recumbent cycles
Recumbent arm-cycles are three wheeled bikes that are controlled with the arms while seated in a reclined position. This type of bicycle has support straps to rest the feet in while cycling.
 Upright cycles
Upright cycles
 Upright cycles
Upright cyclesUpright cycles are similar to recumbent bikes in that the feet are on either side of the front wheel. However, the user is seated in a more upright position when using this bike.
 Tandem bikes
Tandem bikes
 Tandem bikes
Tandem bikesA variety of tandem arm bikes are available. Bike models are available to allow riders to either ride beside each other, or one in front of the other. Power-assist versions are also available for those who may have some function in their legs.
 Arm cycle add-ons
Arm cycle add-ons
 Arm cycle add-ons
Arm cycle add-onsInstead of buying a separate wheelchair, arm-cycle add-ons are available for manual wheelchair users. These add-ons connect to the front of a manual wheelchair, lifting up the casters. This then allows an individual to propel their wheelchair via an arm cycle. Additionally, power-assist versions are available for those with less upper body strength.
Off-road wheelchairs
 If you are looking to go on some trails, an off-road wheelchair may appeal to you. These wheelchairs are used for recreational riding, such as going for a hike, or going fishing. Off-road wheelchairs often have larger, knobbier tires that are meant to withstand the trail, roots, and rocks. Like the arm-cycles, off-road wheelchairs come in a variety of set ups. Some setups may look like a typical manual wheelchair, but with larger wheels. There are also ones that are controlled with push-levers (such as the mountain trike), and powered wheelchairs with more power, suspension, and agility (such as the x5 frontier, and the x8-extreme all-terrain wheelchair).
If you are looking to go on some trails, an off-road wheelchair may appeal to you. These wheelchairs are used for recreational riding, such as going for a hike, or going fishing. Off-road wheelchairs often have larger, knobbier tires that are meant to withstand the trail, roots, and rocks. Like the arm-cycles, off-road wheelchairs come in a variety of set ups. Some setups may look like a typical manual wheelchair, but with larger wheels. There are also ones that are controlled with push-levers (such as the mountain trike), and powered wheelchairs with more power, suspension, and agility (such as the x5 frontier, and the x8-extreme all-terrain wheelchair).
Wheelchair racing

 For those who are interested in competition, wheelchair racing may be an option. Wheelchair race events range from the 100m, 200m, 400m, 800m, 1500m, and 5k distance races in track and field, to marathons. Racing wheelchairs differ from the wheelchairs and cycles listed above in that they typically have two wheels with a third one extended out in front. Ideally, race chairs should be light-weight to enhance performance. When seated, the wheelchair should fit “like a glove”, and there should be little movement in the seat. Unlike arm-cycles, the feet are bent down and kept closer to the body. In addition, specialized rubber gloves are worn to push the rims during races.
For those who are interested in competition, wheelchair racing may be an option. Wheelchair race events range from the 100m, 200m, 400m, 800m, 1500m, and 5k distance races in track and field, to marathons. Racing wheelchairs differ from the wheelchairs and cycles listed above in that they typically have two wheels with a third one extended out in front. Ideally, race chairs should be light-weight to enhance performance. When seated, the wheelchair should fit “like a glove”, and there should be little movement in the seat. Unlike arm-cycles, the feet are bent down and kept closer to the body. In addition, specialized rubber gloves are worn to push the rims during races.
Refer to our article on Wheelchair Propulsion Assist Devices for more information!
Tennis
 Wheelchair tennis is played on the same court as able-bodied tennis, and with similar rules. One rule difference is that in wheelchair tennis, players are allowed two bounces instead of one, and the second bounce can be anywhere – even out of bounds. Although one can play wheelchair tennis in their day chair, tennis wheelchairs are often preferred during play. These wheelchairs are faster, lighter, more agile, and more stable. The wheels on the wheelchair are also angled (i.e., there is more camber ) to allow for more swift turning. For those with limited hand function, taping the racquet to your hand is common practice, though it can take some time to find the optimal tension for you. Therefore, people with all levels of ability can play wheelchair tennis.
Wheelchair tennis is played on the same court as able-bodied tennis, and with similar rules. One rule difference is that in wheelchair tennis, players are allowed two bounces instead of one, and the second bounce can be anywhere – even out of bounds. Although one can play wheelchair tennis in their day chair, tennis wheelchairs are often preferred during play. These wheelchairs are faster, lighter, more agile, and more stable. The wheels on the wheelchair are also angled (i.e., there is more camber ) to allow for more swift turning. For those with limited hand function, taping the racquet to your hand is common practice, though it can take some time to find the optimal tension for you. Therefore, people with all levels of ability can play wheelchair tennis.
 Basketball
Basketball
 Basketball
BasketballWheelchair basketball is played on a standard basketball court. The wheelchair used for basketball is one with wheels angled to 15-20 degrees and a single rollerblade used for a caster at the back. In addition, there are many strapping options to promote stability and safety, or to hold the body in a certain position. Commonly strapped body parts include the hips, knees, feet and/or ankles. It is common for wheelchair basketball leagues to include able bodied participants at the local level of competition. This allows for more players and teams for great league play.
Rugby
 Wheelchair rugby was developed specifically for people with tetraplegia and has grown to include people without SCI but with similar functional abilities (e.g., some impaired arm and hand function in addition to impaired leg function). Wheelchair rugby is played with a volleyball. The goal of the game is to carry the ball over the other team’s goal line. Unlike able-bodied rugby, wheelchair rugby is played indoors on a court. Specialized wheelchairs are used to play wheelchair rugby and can be separated into chairs for offensive players and chairs for defensive players. Offensive wheelchairs are set up for speed and mobility and are distinguished with a front bumper to prevent other chairs from hooking them. Often, offensive chairs are used by players with more function. On the other hand, defensive wheelchairs are set up with a bumper to hook and hold onto other players. Defensive chairs are often used by players with less function. Additional equipment used in rugby include straps and gloves. Straps are used on the waist (to compensate for a lack of core muscles), the thighs (to prevent them from falling to the side or from shifting side to side), and the feet (for comfort). Meanwhile, gloves work to protect the skin, add extra grip when pushing the chair, and to making throwing and catching the ball easier.
Wheelchair rugby was developed specifically for people with tetraplegia and has grown to include people without SCI but with similar functional abilities (e.g., some impaired arm and hand function in addition to impaired leg function). Wheelchair rugby is played with a volleyball. The goal of the game is to carry the ball over the other team’s goal line. Unlike able-bodied rugby, wheelchair rugby is played indoors on a court. Specialized wheelchairs are used to play wheelchair rugby and can be separated into chairs for offensive players and chairs for defensive players. Offensive wheelchairs are set up for speed and mobility and are distinguished with a front bumper to prevent other chairs from hooking them. Often, offensive chairs are used by players with more function. On the other hand, defensive wheelchairs are set up with a bumper to hook and hold onto other players. Defensive chairs are often used by players with less function. Additional equipment used in rugby include straps and gloves. Straps are used on the waist (to compensate for a lack of core muscles), the thighs (to prevent them from falling to the side or from shifting side to side), and the feet (for comfort). Meanwhile, gloves work to protect the skin, add extra grip when pushing the chair, and to making throwing and catching the ball easier.
Community Voices: Byron |

Alpine Skiing

 Alpine skiing, also known as downhill skiing, is a sport that individuals with tetraplegia and paraplegia can partake in with the use of sit-skis. In general, sit skis have a bucket-type of seat with an adjustable seat and footrest. To create a smoother ride, sit-skis have additional features such as suspensions and a shock compression system under the seat. The seat and suspension/shock systems are all connected to either a single ski (mono-ski) or a pair of skis (bi-skis). In general, mono-skis require the user to have good upper body strength, and the ability to ski independently. Bi-skis are often used by individuals who may require some assistance. Often, bi-skis are used with an able-bodied individual who skis behind them. Skiers who use a sit-ski can use the typical chairlifts at the mountains and with experience, can access all terrains of ski areas.
Alpine skiing, also known as downhill skiing, is a sport that individuals with tetraplegia and paraplegia can partake in with the use of sit-skis. In general, sit skis have a bucket-type of seat with an adjustable seat and footrest. To create a smoother ride, sit-skis have additional features such as suspensions and a shock compression system under the seat. The seat and suspension/shock systems are all connected to either a single ski (mono-ski) or a pair of skis (bi-skis). In general, mono-skis require the user to have good upper body strength, and the ability to ski independently. Bi-skis are often used by individuals who may require some assistance. Often, bi-skis are used with an able-bodied individual who skis behind them. Skiers who use a sit-ski can use the typical chairlifts at the mountains and with experience, can access all terrains of ski areas.
 Cross Country Skiing
Cross Country Skiing
 Cross Country Skiing
Cross Country SkiingCross country skiing (which is a type of Nordic skiing) allows individuals with paraplegia and tetraplegia to explore snowy trails. Like the alpine skis, cross country skis consist of a bucket seat that connects to a metal frame, which clips into the skis. Cross country skiers also often use poles while skiing to propel themselves along flatter terrain. If assistance is required, an able-bodied person can help push the ski forward with their ski-pole using an adaptive add-on.
 Sledge (Ice) Hockey
Sledge (Ice) Hockey
 Sledge (Ice) Hockey
Sledge (Ice) HockeySledge hockey, or para ice hockey is identical to ice hockey but is played while sitting in sledges as opposed to standing on skates.
A sledge consists of a plastic bucket-shaped seat that is connected to a metal frame. This frame is set on two adjustable skate blades, with the blades aligned on the bottom of the seat. The skate blades may be adjusted so that they are further apart for stability (good for new players) or can be moved closer together to allow for more maneuverability and speed. Straps are available to help keep the feet, knees, and hips in place. Players propel themselves in the sledge using two sticks. These sticks are dual ended: one end has a blade for handling the puck, while the other end has a metal pick in it to help players propel themselves across the ice. Typical hockey pads are used for safety during play.
Sailing
Adapted sailing is a sport that people of all abilities can participate in. Common features of adapted sailboats include handguards along the side of the boats, greater deck space due to removed masts, and customized molded seats with back support and belts that pivot. For individuals with reduced function, other available adaptations include electronic controls (such as the use of a joystick), and sip ‘n’ puff technology to steer the boat with breath. Many sailing clubs have power/mechanical lifts dockside to assist with transfers into boats.
|
 Community Voices: Terry
Community Voices: TerryKayaking

 Kayaks are available for people with all levels of SCI. While individuals with a lower level of injury may use non-adapted kayaks, adaptations are available for comfort and to accommodate those with limited function. Some kayaks may have custom seating with side and abdominal support. These supports are cushioned to protect the skin while kayaking. Stabilizing outriggers are available to increase stability of the boat and to reduce the chances of tipping. For those with limited arm/hand function, there are various adaptations for the paddle including:
Kayaks are available for people with all levels of SCI. While individuals with a lower level of injury may use non-adapted kayaks, adaptations are available for comfort and to accommodate those with limited function. Some kayaks may have custom seating with side and abdominal support. These supports are cushioned to protect the skin while kayaking. Stabilizing outriggers are available to increase stability of the boat and to reduce the chances of tipping. For those with limited arm/hand function, there are various adaptations for the paddle including:
- A back of the hand grip, which places more paddling pressure on the arms instead of the hands.
- Wrist cuff adaptation, which allows individuals to connect the paddle to their wrists via a cuff.
There are many benefits to staying physically active after SCI and there is a large variety of sports to participate in. Whether you prefer staying on land, floating on water, or being in the snow, most sports have been adapted in some way or another so that all who want to can participate! Prior to trying a sport, talk with your health providers to ensure that you are in a condition to play.
Evidence for “Why be physically active after SCI” is based on:
Martin KA, Latimer AE, Francoeur C, Hanley H. Sustaining exercise motivation and participation among people with spinal cord injuries – Lessons learned from a 9 month intervention. Palaestra 2002;18(1):38-51.
Hicks AL, Martin KA, Ditor DS, Latimer AE, Craven C, Bugaresti J et al. Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord 2003;41(1):34-43.
Latimer AE, Ginis KA, Hicks AL, McCartney N. An examination of the mechanisms of exercise- induced change in psychological well-being among people with spinal cord injury. J Rehabil Res Dev 2004;41(5):643-652.
Martin Ginis KA, Latimer AE, McKechnie K, Ditor DS, Hicks AL, Bugaresti J. Using exercise to enhance subjective well-being among people with spinal cord injury: The mediating influences of stress and pain. REHABIL PSYCHOL 2003;48(3):157-164.
Latimer AE, Martin Ginis KA, Hicks AL. Buffering the effects of stress on well-being among individuals with spinal cord injury: A potential role for exercise. Therapeutic Recreation Journal 2005;39(2):131-138.
Mulroy, S. J., Thompson, L., Kemp, B., Hatchett, P. P., Newsam, C. J., Lupold, D. G., et al. (2011). Strengthening and Optimal Movements for Painful Shoulders (STOMPS) in chronic spinal cord injury: a randomized controlled trial. Physical Therapy, 91, 305—324.
Jacobs, P. L. (2009). Effects of resistance and endurance training in persons with paraplegia. Medicine & Science in Sports & Exercise, 41, 992-997.
De Groot PC, Hjeltnes N, Heijboer AC, Stal W, Birkeland K. Effect of training intensity on physical capacity, lipid profile and insulin sensitivity in early rehabilitation of spinal cord injured individuals. Spinal Cord 2003;41(12):673-679.
de Carvalho DC, Martins CL, Cardoso SD, Cliquet A. Improvement of metabolic and cardiorespiratory responses through treadmill gait training with neuromuscular electrical stimulation in quadriplegic subjects. Artif Organs 2006;30(1):56-63.
Information for “What are adapted sports” is based on:
World Para Athletes. (n.d.). What is classification? https://www.paralympic.org/athletics/classification
Information for “What types of cycling and pushing sports are there?” is based on:
World Para Athletes. (n.d.). Para-athletics explained: Wheelchair racing. https://www.paralympic.org/news/para-athletics-explained-wheelchair-racing
Chair Institute. (2019). Best off road all terrain wheelchairs for outdoors review 2020. https://chairinstitute.com/best-wheelchairs-for-outdoors/
Information for “What adapted court sports are available?” is based on:
BC Wheelchair Sports. (n.d.). Wheelchair Tennis.https://www.bcwheelchairsports.com/sites/default/files/images/BCWSA%20Wheelchair%20Tennis%20First%20Introduction%20Manual%20-%20PRINT%20%281%29.pdf
Wheelchair Basketball Canada. (2021). About the sport. https://www.wheelchairbasketball.ca/the-sport/about-the-sport/
Wheelchair Basketball Canada. (2021). Equipment. https://www.wheelchairbasketball.ca/the-sport/equipment/
Wheelchair Rugby Canada. (2018). Rules and equipment. https://wheelchairrugby.ca/rules-equipment/
Information for “What adapted winter sports are available?” is based on:
Canadian Ski Council. (2018). Skiing is for everyone! https://www.skicanada.org/ready/accessible-skiing-information/
XCSkiResorts. (2016). Nordic adaptive sit-skis bring freedom to mobility impaired persons. https://www.xcskiresorts.com/resort-features/2016/9/12/nordic-adaptive-sit-skis-bring-freedom-to-mobility-impaired-persons
BC Hockey – Saanichton, BC. (2016). Para Hockey Brochure Guide.https://www.bchockey.net/Files/Sledge%20Hockey%20Brochure.pdf
Information for “What water sports are available?” is based on:
Move United. (n.d.). Sailing. https://www.moveunitedsport.org/sport/sailing/
Disabled Sailing Association of British Columbia. (2021). Sip ‘n’ Puff Technology. https://asabc.org/sip-n-puff/
Creating Ability. (2021). Seating systems. https://www.creatingability.com/seating-systems/
Creating Ability. (2021). Paddle adaptations. https://www.creatingability.com/paddle-adaptations/
Image credits
- Man on Arm Erg by SCIRE Community
- BC Wheelchair Rugby Day 1 293©Melissa Nemeth, CC BY-SA 2.0
- Noun Project
- Noun Project
- Noun Project
- Shark ©Sunrise Medical 2021
- Replacement parts for Invacare Top End Handcycles ©RehabMart.com, LLC 1998-2021
- Van Ram Fun2Go Tandem ©Bike-On.com 2020
- Batec Hybrid ©Batec Mobility
- Invacare top end crossfire all terrain wheelchair ©Invacare Corporation 2021
- Top end preliminator youth racing wheelchair – custom version. ©How I Roll Sports, LLC 2018
- Harness Glove ©Harness Designs Wheelchair Gloves
- Wheelchair Tennis ©BC Wheelchair Sports
- Wigan Warthogs Wheelchair Basketball-2 ©Andrew Spillane, CC BY-ND 2.0
- Equipment ©International Wheelchair Rugby Federation 2013-2021
- London 2012 Paralympics Wheelchair Rugby (Murderball) ©Sum_of_Marc, CC BY-NC-ND 2.0
- Monique-1 Mono Ski ©Enabling Technologies 2021
- Dynamique Bi Ski ©Enabling Technologies 2021
- Woman using sit ski – photo by northeast passage ©U.S. Forest Service – Pacific Northwest Region, Public Domain Mark 1.0
- Sledge Hockey: Italy/Sweden ©Mariska Richters, CC BY-NC-SA 2.0
- Terry in Matin 16
- Outfitted Kayak ©Creating Ability 2021
- Stabilizing Outriggers ©Creating Ability 2021








 For gel cushions: knead the gel from outside to inside. Ensure that the gel is redistributed, and that gel is present under areas of high pressure (e.g., in the area of your sit bones). In addition, ensure that there are no leaks in your cushion.
For gel cushions: knead the gel from outside to inside. Ensure that the gel is redistributed, and that gel is present under areas of high pressure (e.g., in the area of your sit bones). In addition, ensure that there are no leaks in your cushion.

 Spokes are attached from the wheel rim (outer part of the wheel) to the hub (center part of the wheel), and help to distribute the forces of wheeling, such as the weight of the user, wheeling over surfaces, and braking. The spokes on a wheel act to prevent the tire from collapsing and adds stiffness to a wheel by acting as an anchor for the hub of the wheel.
Spokes are attached from the wheel rim (outer part of the wheel) to the hub (center part of the wheel), and help to distribute the forces of wheeling, such as the weight of the user, wheeling over surfaces, and braking. The spokes on a wheel act to prevent the tire from collapsing and adds stiffness to a wheel by acting as an anchor for the hub of the wheel.


 Like the rear wheel, casters consist of wheel bearings to ensure smooth rolling. To check that the bearings are at a happy medium in tension, spin the caster wheels and the caster assembly, and push the caster side to side. Grinding and excessive play in the caster bearings are indicative of a problem.
Like the rear wheel, casters consist of wheel bearings to ensure smooth rolling. To check that the bearings are at a happy medium in tension, spin the caster wheels and the caster assembly, and push the caster side to side. Grinding and excessive play in the caster bearings are indicative of a problem.

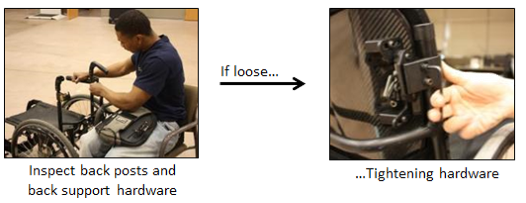 As the backrest is used to support your sitting posture and can impact your skin health, it is important to check that it is in good shape. To do so, check the upholstery for tears, wear, stretching, or metal parts that have poked through. If you have a rigid back, check that the backrest does not wiggle and is tightly secured. In addition, make sure that the backrest height is level. It is possible for a backrest bracket to become loose, resulting in one side of the backrest being higher than the other.
As the backrest is used to support your sitting posture and can impact your skin health, it is important to check that it is in good shape. To do so, check the upholstery for tears, wear, stretching, or metal parts that have poked through. If you have a rigid back, check that the backrest does not wiggle and is tightly secured. In addition, make sure that the backrest height is level. It is possible for a backrest bracket to become loose, resulting in one side of the backrest being higher than the other. Maintaining a power wheelchair may seem intimidating given the integration of electronics, but most activities are fairly simple. Below we discuss the tasks you should complete with your wheelchair.
Maintaining a power wheelchair may seem intimidating given the integration of electronics, but most activities are fairly simple. Below we discuss the tasks you should complete with your wheelchair. Shrouds are the plastic coverings that protect the electronics and the battery of the wheelchair from dirt and moisture. To check them, make sure that they are present and intact. Try to jiggle the shrouds around to ensure they are not loose.
Shrouds are the plastic coverings that protect the electronics and the battery of the wheelchair from dirt and moisture. To check them, make sure that they are present and intact. Try to jiggle the shrouds around to ensure they are not loose. Turn down the speed of your wheelchair
Turn down the speed of your wheelchair The treads on your tire play a key role in maintaining traction and maintaining the stability and maneuverability of the wheelchair. Some tires may have less tread than others; note how much tread your tire starts off with. Check the tire treads monthly to ensure that they are not worn.
The treads on your tire play a key role in maintaining traction and maintaining the stability and maneuverability of the wheelchair. Some tires may have less tread than others; note how much tread your tire starts off with. Check the tire treads monthly to ensure that they are not worn. The axles of the front caster wheels of the wheelchair are the lowest to the ground, and thus are susceptible to picking up hair, dust, lint, and dirt. Buildup on your axles can lead to premature wearing and increased rolling resistance. For example, hair wrapped around the caster wheel can lead to breakage. Using a pair of scissors, tweezers, a toothbrush, or pliers, remove debris from the caster.
The axles of the front caster wheels of the wheelchair are the lowest to the ground, and thus are susceptible to picking up hair, dust, lint, and dirt. Buildup on your axles can lead to premature wearing and increased rolling resistance. For example, hair wrapped around the caster wheel can lead to breakage. Using a pair of scissors, tweezers, a toothbrush, or pliers, remove debris from the caster.










 These light-weight durable cushions resemble a honeycomb in that they are composed of multiple open cells. These cells are able to distribute pressure evenly while avoiding the risk of being punctured. Air flow is also promoted throughout the open cells to prevent skin breakdown. As these cushions are made out of urethane, a material that resembles rubber, they also provide good shock absorbance. However, compared to other cushions, they provide moderate positioning capabilities and are not modifiable in shape.
These light-weight durable cushions resemble a honeycomb in that they are composed of multiple open cells. These cells are able to distribute pressure evenly while avoiding the risk of being punctured. Air flow is also promoted throughout the open cells to prevent skin breakdown. As these cushions are made out of urethane, a material that resembles rubber, they also provide good shock absorbance. However, compared to other cushions, they provide moderate positioning capabilities and are not modifiable in shape. Flat backrests are flat or slightly curved in shape, and often consist of a stiff flat surface (e.g., plastic, plywood) that is layered with foam and covered with material. This style of back allows for the greatest range of motion of the arms, thus creating increased freedom. Another advantage of the flat backrest is that it is very adjustable and can accommodate a large variety of support accessories, such as lateral supports, chest straps, and headrests. A drawback to this style of back is that it provides limited support. It does not accommodate for the shape of the spine, making it less suitable for individuals with lordosis (i.e., sway back) or kyphosis (i.e., a hunched back).
Flat backrests are flat or slightly curved in shape, and often consist of a stiff flat surface (e.g., plastic, plywood) that is layered with foam and covered with material. This style of back allows for the greatest range of motion of the arms, thus creating increased freedom. Another advantage of the flat backrest is that it is very adjustable and can accommodate a large variety of support accessories, such as lateral supports, chest straps, and headrests. A drawback to this style of back is that it provides limited support. It does not accommodate for the shape of the spine, making it less suitable for individuals with lordosis (i.e., sway back) or kyphosis (i.e., a hunched back). General contoured backrests are off-the-shelf backs that are shaped, but are not customized to your back. These backs provide more support than a flat back, as they have a deeper contour that can provide lateral (side) support. The effectiveness of general contoured backs is based on how well the back fits your needs; they may only be effective if you can find one that suits your needs.
General contoured backrests are off-the-shelf backs that are shaped, but are not customized to your back. These backs provide more support than a flat back, as they have a deeper contour that can provide lateral (side) support. The effectiveness of general contoured backs is based on how well the back fits your needs; they may only be effective if you can find one that suits your needs. Custom contoured backs provide increased support for positioning, and are made custom to the shape of your back. This cushion is often used if you require extra positioning support, and if the general control back or flat back does not meet your needs. The creation of custom contour backs can be a lengthy and costly labour-intensive process. When creating a custom contour back, a mold of your back is taken. A seating specialist then inspects the mold to ensure that it is reflective of the shape of your back and that the contour information is accurate. The backrest is then carefully made to the specifications obtained from the measuring process. As custom contour backs are designed to fit the shape of your back to provide more support, they also impose limitations on flexibility. When transferring in and out of your wheelchair, it is also important to be properly aligned in your custom contoured backrest, as improper fitting may lead to pressure sores or skin breakdown.
Custom contoured backs provide increased support for positioning, and are made custom to the shape of your back. This cushion is often used if you require extra positioning support, and if the general control back or flat back does not meet your needs. The creation of custom contour backs can be a lengthy and costly labour-intensive process. When creating a custom contour back, a mold of your back is taken. A seating specialist then inspects the mold to ensure that it is reflective of the shape of your back and that the contour information is accurate. The backrest is then carefully made to the specifications obtained from the measuring process. As custom contour backs are designed to fit the shape of your back to provide more support, they also impose limitations on flexibility. When transferring in and out of your wheelchair, it is also important to be properly aligned in your custom contoured backrest, as improper fitting may lead to pressure sores or skin breakdown.


 Using armrests can help maintain a good seated posture for an individual using a wheelchair. By supporting the arms and forearms, weight is alleviated from the shoulders. Without armrests, the weight of your arms may pull your shoulder down, resulting in a hunched position. It is also important that your armrests are set to an appropriate height. Armrests that are too low may require the individual to lean forward to use the armrest, which may lead to hunching. If the armrests are too high, the shoulders may be pushed up too high, which can lead to discomfort.
Using armrests can help maintain a good seated posture for an individual using a wheelchair. By supporting the arms and forearms, weight is alleviated from the shoulders. Without armrests, the weight of your arms may pull your shoulder down, resulting in a hunched position. It is also important that your armrests are set to an appropriate height. Armrests that are too low may require the individual to lean forward to use the armrest, which may lead to hunching. If the armrests are too high, the shoulders may be pushed up too high, which can lead to discomfort., depicting the action of two different mobility-challenged women getting into a bathtub ©Richard Duncan, Public Domain") Armrests can act as a source of support for repositioning to alleviate pressure on the sit bones. Weak evidence suggests that individuals with paraplegia rely on armrests more than tetraplegics during weight shifting (9% of their body weight vs 5%). The researchers think that this may be the case because individuals with tetraplegia have weak arm extensor muscles, making weight relieving difficult. In addition to acting as a support to push off from, armrests can also help alleviate pressure on the sit bones by supporting the weight of your arms. By removing the weight of hanging arms, the hips are unloaded and pressure forces are redistributed.
Armrests can act as a source of support for repositioning to alleviate pressure on the sit bones. Weak evidence suggests that individuals with paraplegia rely on armrests more than tetraplegics during weight shifting (9% of their body weight vs 5%). The researchers think that this may be the case because individuals with tetraplegia have weak arm extensor muscles, making weight relieving difficult. In addition to acting as a support to push off from, armrests can also help alleviate pressure on the sit bones by supporting the weight of your arms. By removing the weight of hanging arms, the hips are unloaded and pressure forces are redistributed.
 2015")
 2015") Various accessories are available to help support and position all parts of the lower limb including: the hips and buttock, knees, lower legs, and feet. To support the hips and the buttock, positioning belts (sometimes referred to as seat belts) can be used. When used on wheelchairs, positioning belts can help prevent the hips from sliding forward and help to keep the hips properly aligned (i.e., not tilted or rotated). Different types of positioning belts are available depending on your needs: two-point belts or four-point belts. Four-point belts offer more support to the hips if required. It is also important to note that safety belts are not the same as positioning belts. Although both may contribute towards safety, positioning belts are more specialized to help maintain your hip posture.
Various accessories are available to help support and position all parts of the lower limb including: the hips and buttock, knees, lower legs, and feet. To support the hips and the buttock, positioning belts (sometimes referred to as seat belts) can be used. When used on wheelchairs, positioning belts can help prevent the hips from sliding forward and help to keep the hips properly aligned (i.e., not tilted or rotated). Different types of positioning belts are available depending on your needs: two-point belts or four-point belts. Four-point belts offer more support to the hips if required. It is also important to note that safety belts are not the same as positioning belts. Although both may contribute towards safety, positioning belts are more specialized to help maintain your hip posture.








 There are some devices that facilitate pushing by amplifying your efforts (a mechanical advantage) using gears or levers. Using a device with a mechanical advantage will allow you to go further with a given push. One example of a device that provides mechanical advantage is a lever-propelled wheelchair. There are some lever devices that can be connected to your wheel (others require replacement of the rear wheels) that allow the user to propel by pushing the lever forward. Using a lever has two purported benefits: 1) using a longer lever to propel a wheelchair requires less force, and 2) using a lever enables a more favorable movement pattern of the hands, wrists, and shoulder. Together these may reduce the risk of injury. An example of this device is the NuDrive.
There are some devices that facilitate pushing by amplifying your efforts (a mechanical advantage) using gears or levers. Using a device with a mechanical advantage will allow you to go further with a given push. One example of a device that provides mechanical advantage is a lever-propelled wheelchair. There are some lever devices that can be connected to your wheel (others require replacement of the rear wheels) that allow the user to propel by pushing the lever forward. Using a lever has two purported benefits: 1) using a longer lever to propel a wheelchair requires less force, and 2) using a lever enables a more favorable movement pattern of the hands, wrists, and shoulder. Together these may reduce the risk of injury. An example of this device is the NuDrive. A PAPAW is a manual wheelchair with motorized rear wheels. The wheels are powered by a battery, which is attached to the back of the wheelchair. This type of wheelchair is controlled by normal pushing movements using the pushrims. PAPAWs assist individuals with limited strength or arm function by amplifying the force applied to the wheels. Each push on the pushrim by the user is sensed and proportionally amplified to increase the force to continue the forward movement. This also occurs for braking and turning (e.g., the wheels would detect a backwards force and apply a stronger braking force). This allows for users to go further with a given push, or to brake more efficiently with less force. When desired, the power assist function can be turned off. One limitation of using PAPAWs is the significantly increased weight of the wheelchair, which is especially noticeable when turned off. Another limitation is that the pushrims are damaged more easily, as this is where the sensors are located. Some examples of PAPAWs include the Alber E-motion and the Quickie Xtender.
A PAPAW is a manual wheelchair with motorized rear wheels. The wheels are powered by a battery, which is attached to the back of the wheelchair. This type of wheelchair is controlled by normal pushing movements using the pushrims. PAPAWs assist individuals with limited strength or arm function by amplifying the force applied to the wheels. Each push on the pushrim by the user is sensed and proportionally amplified to increase the force to continue the forward movement. This also occurs for braking and turning (e.g., the wheels would detect a backwards force and apply a stronger braking force). This allows for users to go further with a given push, or to brake more efficiently with less force. When desired, the power assist function can be turned off. One limitation of using PAPAWs is the significantly increased weight of the wheelchair, which is especially noticeable when turned off. Another limitation is that the pushrims are damaged more easily, as this is where the sensors are located. Some examples of PAPAWs include the Alber E-motion and the Quickie Xtender.
 Rear mounted propulsion device generally connect to the bar underneath the wheelchair seat (i.e., the camber tube). These devices can power the wheelchair so that no manual propulsion is required, although turning and braking still require constant user control. Currently, there are two models commercially available that are light, compact, and easily attached: the SmartDrive and the Smoov. The SmartDrive is controlled with a wristband worn by the user. A double tap of the wristband (or similar accelerometer-sensed motion of the hand/arm when tapping the wheel or other surface) will activate the motor and begin accelerating the wheelchair. Another tap sets the speed, while the next double tap will stop the motor. Gripping on the handrim is usually still needed to slow down and stop the chair. Users are not required to propel the wheelchair once it is in motion; they are only required to steer. Good reaction time is required to operate the device; a learning curve is involved when first using the device. The Smoov operates via a frame mounted control knob to set the desired speed. Starting and stopping the motor is accomplished through tapping the knob. Turning, slowing, and stopping are similar to the SmartDrive operation.
Rear mounted propulsion device generally connect to the bar underneath the wheelchair seat (i.e., the camber tube). These devices can power the wheelchair so that no manual propulsion is required, although turning and braking still require constant user control. Currently, there are two models commercially available that are light, compact, and easily attached: the SmartDrive and the Smoov. The SmartDrive is controlled with a wristband worn by the user. A double tap of the wristband (or similar accelerometer-sensed motion of the hand/arm when tapping the wheel or other surface) will activate the motor and begin accelerating the wheelchair. Another tap sets the speed, while the next double tap will stop the motor. Gripping on the handrim is usually still needed to slow down and stop the chair. Users are not required to propel the wheelchair once it is in motion; they are only required to steer. Good reaction time is required to operate the device; a learning curve is involved when first using the device. The Smoov operates via a frame mounted control knob to set the desired speed. Starting and stopping the motor is accomplished through tapping the knob. Turning, slowing, and stopping are similar to the SmartDrive operation. Other rear-mounted systems, such as the Spinergy ZX-1, convert manual wheelchairs into a power wheelchair. The user backs up into the device, which connects to the wheelchair with a push of the button. This add-on lifts up the rear wheels of the wheelchair, converting it into a power wheelchair that is controlled with a joystick.
Other rear-mounted systems, such as the Spinergy ZX-1, convert manual wheelchairs into a power wheelchair. The user backs up into the device, which connects to the wheelchair with a push of the button. This add-on lifts up the rear wheels of the wheelchair, converting it into a power wheelchair that is controlled with a joystick.





 The characteristics of your mobility device can also affect how you function in day-to-day life. For example, small tweaks to your wheelchair set-up can make it easier or more difficult to maneuver and propel yourself. The characteristics of your device may also affect the environments and situations that you can use it in, such as whether it can be used outside, during sports, or can be put in and out of a car independently.
The characteristics of your mobility device can also affect how you function in day-to-day life. For example, small tweaks to your wheelchair set-up can make it easier or more difficult to maneuver and propel yourself. The characteristics of your device may also affect the environments and situations that you can use it in, such as whether it can be used outside, during sports, or can be put in and out of a car independently. There are a variety of styles of wheelchairs and scooters, each with their own benefits and drawbacks. Properties of various mobility devices, such as the turning radius, the length and width, and the stability of the device may impact the types of activities that a wheelchair user can participate in. For example, a wheelchair that has a wide turning radius may not be able to maneuver in smaller stores with narrow aisles. Additionally, some devices perform better in inclement weather than others. This may be a consideration for individuals living in areas where it is often rains or snows.
There are a variety of styles of wheelchairs and scooters, each with their own benefits and drawbacks. Properties of various mobility devices, such as the turning radius, the length and width, and the stability of the device may impact the types of activities that a wheelchair user can participate in. For example, a wheelchair that has a wide turning radius may not be able to maneuver in smaller stores with narrow aisles. Additionally, some devices perform better in inclement weather than others. This may be a consideration for individuals living in areas where it is often rains or snows.





")
")
") Standing
Standing








 Folding wheelchairs are designed to be folded vertically and take up minimal storage space. This allows for easy portability (such as fitting the wheelchair into a car). However, these wheelchairs also have many moving parts that may break down or loosen over time, and are heavier than rigid wheelchairs. Folding wheelchair often have flip up, swing away or swing in footrests so they may be used by individuals that do not use the wheelchair full time, can stand or take some steps, or by those who foot propel.
Folding wheelchairs are designed to be folded vertically and take up minimal storage space. This allows for easy portability (such as fitting the wheelchair into a car). However, these wheelchairs also have many moving parts that may break down or loosen over time, and are heavier than rigid wheelchairs. Folding wheelchair often have flip up, swing away or swing in footrests so they may be used by individuals that do not use the wheelchair full time, can stand or take some steps, or by those who foot propel. ©Memasa CC BY-SA 3.0")












 Propulsion pattern: the pattern you push your wheelchair with (e.g., where do your hands go when you push and after you’re done pushing) may also have an influence on your risk of injury. Some weak evidence suggests that using the semi-circular and double-loop-over may reduce the risk of nerve injury and are the most optimal ways to push your wheelchair. Further evidence (weak) has indicated that arcing may be more efficient for short bouts of high intensity pushing (like when going uphill).
Propulsion pattern: the pattern you push your wheelchair with (e.g., where do your hands go when you push and after you’re done pushing) may also have an influence on your risk of injury. Some weak evidence suggests that using the semi-circular and double-loop-over may reduce the risk of nerve injury and are the most optimal ways to push your wheelchair. Further evidence (weak) has indicated that arcing may be more efficient for short bouts of high intensity pushing (like when going uphill).
.")



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}